
Pharmaceutical companies invest heavily in three core engagement channels: product reps, MSLs and digital content. The usual assumption is that if a channel performs well overall, it should be rolled out more widely.
Our 2026 So What? Doctor Engagement Barometer shows what that assumption can miss. The same MSL visit that earns a 90% “good or great” rating from medical oncologists earns 54% from psychiatrists. The same digital content a GP finds useful is rated average or poor by many medical oncologists.
Channel value is not fixed. It depends on who receives it, in what context, and whether it meets a real clinical need. A channel that performs strongly in one specialty can underperform in another.
In this article, we explore:
For brand teams planning 2027, the key question is which channel is best for which doctor and whether current channel mix reflects that.
We asked 500 Australian doctors to rate the value of three core pharma channels: product rep visits, MSL visits, and digital content (emails, websites, online content).
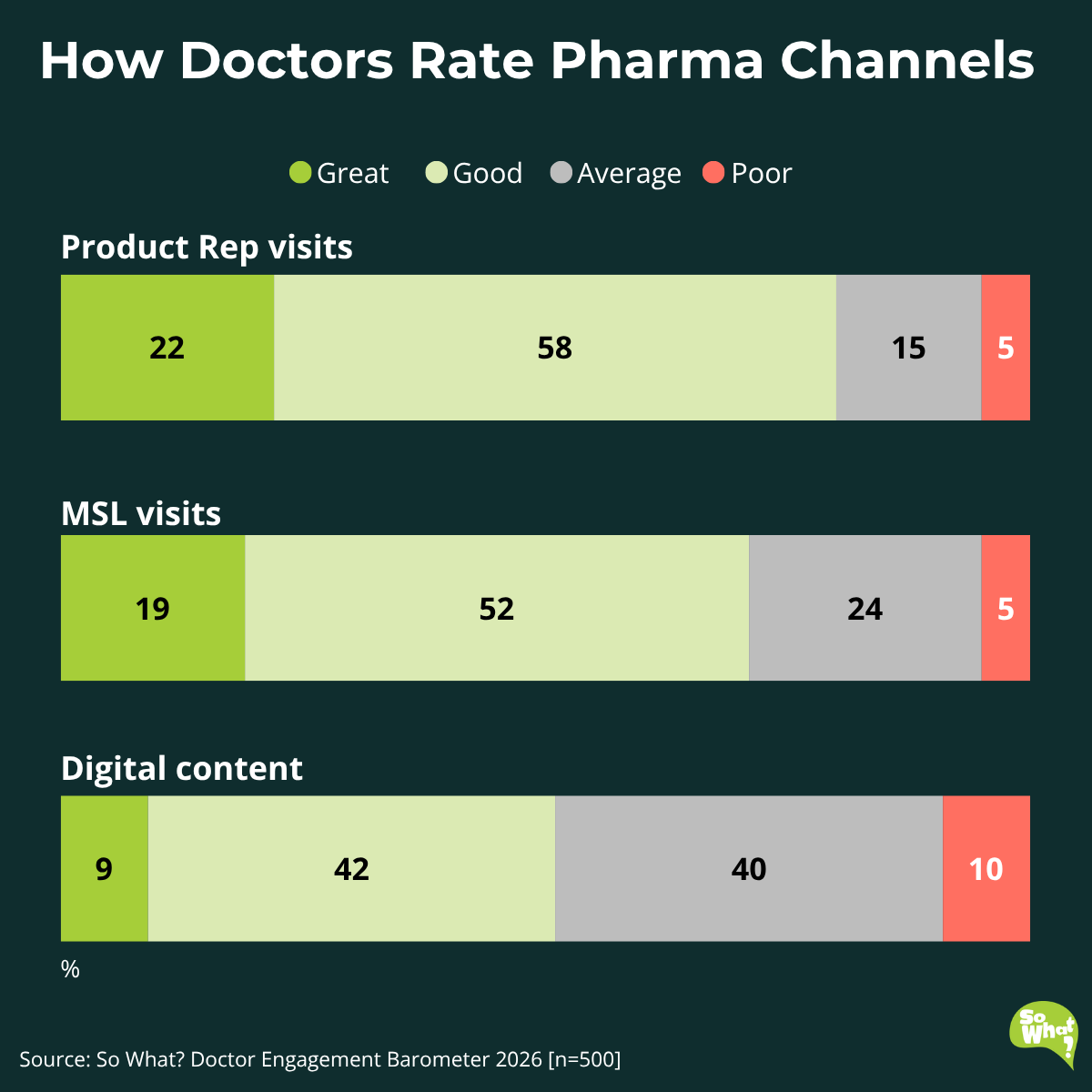
The results show a clear hierarchy:
Rep visits lead while digital content lags well behind. MSLs sit in the middle but only among doctors they reach.
MSLs deliver the strongest value where scientific exchange is most relevant.
.png)
Among medical oncologists, 90% rate MSL visits as “good or great”, the highest score for any doctor group in the dataset. At the other end, only 54% of psychiatrists and 53% of rheumatologists say the same.
The variation suggests MSL value is highly dependent on where the role is deployed. MSLs create the most value in specialties shaped by scientific complexity, active trial landscapes and high-stakes treatment decisions. Where that fit is weaker, value drops.
Among GPs who do interact with MSLs, 77% rate those visits “good or great”, versus 67% of specialists overall.
The most likely explanation is selection: these are not typical GPs, but GPs with information needs beyond what a rep visit provides. When those GPs get access to MSLs, they value it.
Digital content performs better with GPs than with specialists.
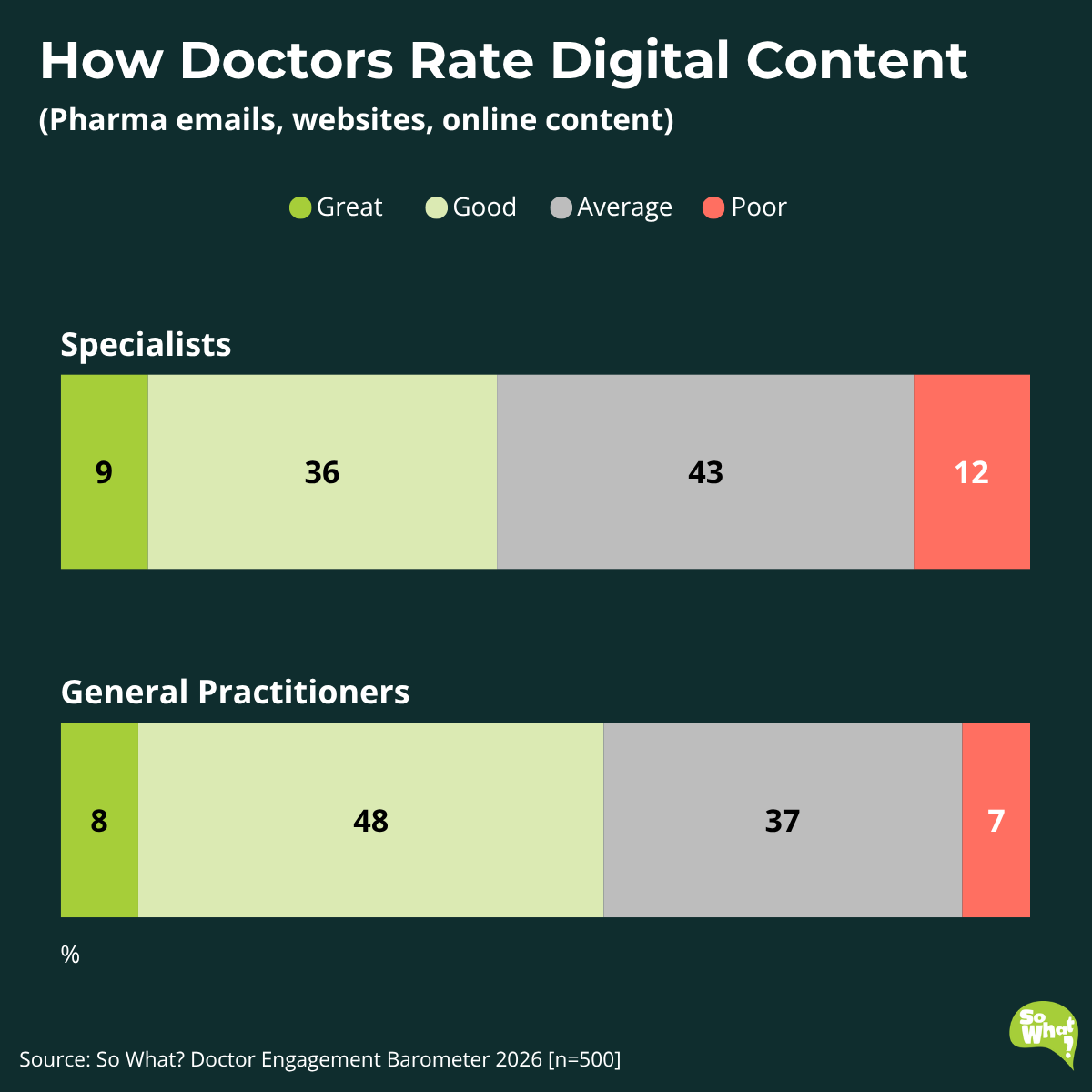
In the chart above, 56% of GPs rate pharma digital content “good or great”, compared with 45% of specialists. Specialists are also more likely to rate it “average or poor”, suggesting digital content is working less well for specialist audiences.
That broader specialist picture helps explain why some specialties are particularly dissatisfied. Among medical oncologists, only 32% rate digital content “good or great”, while 68% rate it “average or poor”, the lowest result of any specialty in the dataset.
Across the full sample, only 9% of doctors rate pharma digital content as “great”. For a channel absorbing a growing share of budget, that is a weak result.
The assumption that younger doctors are more receptive to pharma digital content is not supported by the data. Among Millennials, 47% rate digital content “good or great”, compared with 53% of Baby Boomers.
If your digital strategy assumes that the next generation of prescribers will naturally be more receptive to digital, this data suggests otherwise. This points back to content value rather than age-based assumptions about channel preference.
We asked doctors whether they wanted to keep the current balance of rep and MSL support, or shift it towards more reps, more MSLs, or more of both.
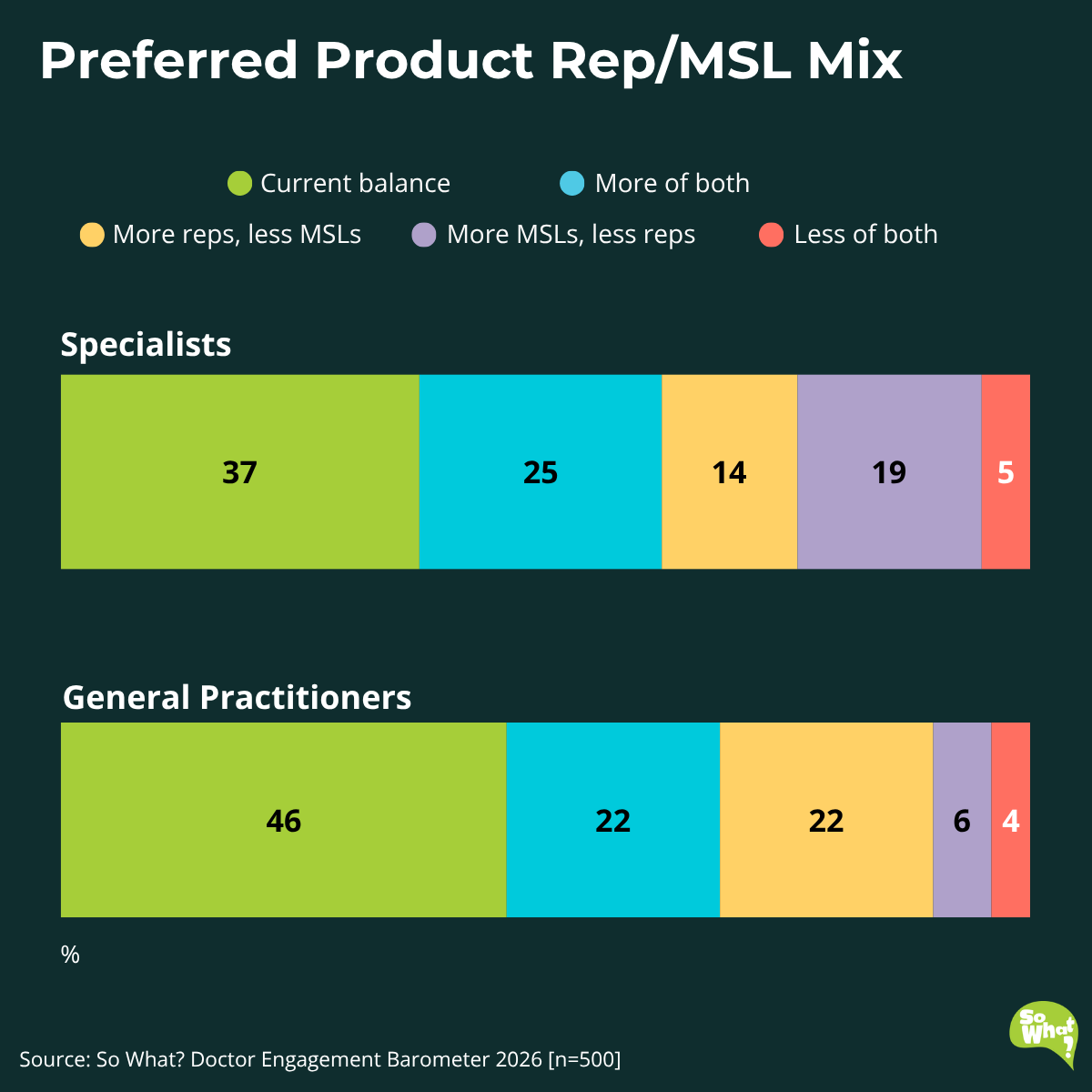
The graph shows a clear split between GPs and specialists. GPs are more likely to want to keep the current balance (46% vs 37%) and more likely to want more reps and fewer MSLs (22% vs 14%). Specialists are more likely to want more MSLs and fewer reps (19% vs 6%) and slightly more likely to want more of both roles (25% vs 22%).
The broader picture is still one of an appetite for pharma engagement. Only 4% of GPs and 5% of specialists say they want less of both roles.
Within specialists, the average hides further variation. Medical oncologists show the strongest preference for more MSLs and fewer reps (39%) while psychiatrists the strongest preference for more of both roles (37%), suggesting they feel underserved overall.
A single national rep/MSL ratio is unlikely to fit most specialties. A better model is one calibrated to the needs of each audience.
These findings point to four priorities for engagement channel planning:
1. Calibrate MSL focus by specialty
The 36-point gap between medical oncologists and psychiatrists suggests MSL value varies sharply by specialty.
2. Rebuild digital content around clinical utility
The issue is value. Pharma is getting digital content in front of doctors, but too often it is not meeting their needs especially in high-priority specialties such as oncology.
3. Challenge the assumption that younger doctors are more digitally receptive
Millennials rate pharma digital content lower than Baby Boomers, so age alone is a weak guide for digital planning.
4. Build field force models by specialty, not at national average
Different specialties want different balances of rep and MSL support. A single national model risks misalignment across multiple audiences at once.
Three questions to take into your next planning meeting:
1. Are our MSLs focused where they create the most value?
Compare current MSL coverage with specialty-level value. Where is support well aligned, and where are high-value audiences being missed?
2. Is our digital content genuinely useful in practice?
For priority specialties, the bar is clinical utility not simply turning promotional messages into digital assets.
3. Are we using the right product rep vs MSL mix by specialty?
The variation in preference is large enough to affect resource allocation. A single national model is unlikely to be the right answer.
These findings provide a national benchmark. What they do not show is whether your own channel mix, MSL targeting and digital strategy are aligned to the needs of your priority customers.
If you’d like to explore what this means for your therapy area, contact us today.
These insights come from The So What? Doctor Engagement Barometer 2026, an independent national online study of 500 Australian doctors (250 GPs and 250 specialists across 20+ specialties). Fieldwork was conducted from December 2025 to February 2026.
.svg)
